Baby Percentile During Pregnancy: What Ultrasound Percentiles Mean (2026)
Baby percentile during pregnancy shows fetal size vs. same-age fetuses on ultrasound. How it's calculated, what SGA means, and what helps improve fetal growth.
The 20-week anatomy scan is the first time most parents hear a percentile attached to their baby. The sonographer types a few measurements into the machine, it runs a calculation, and the printout says "Estimated Fetal Weight: 340 grams, 42nd percentile." The appointment moves on. You leave with a number you were not prepared to interpret.
Baby percentile during pregnancy means something different from the percentile your pediatrician tracks after birth. The postnatal Baby Percentile Calculator uses WHO growth standards and direct weight measurements. Fetal percentile is estimated differently: it uses ultrasound-derived measurements and a separate fetal reference population, with a known error margin that postnatal measurements do not carry. Understanding that gap prevents a lot of unnecessary confusion when a fetus reads "32nd percentile" on the scan and then arrives at the 55th percentile on the WHO chart after birth.
How Fetal Weight Percentile Is Estimated During Pregnancy
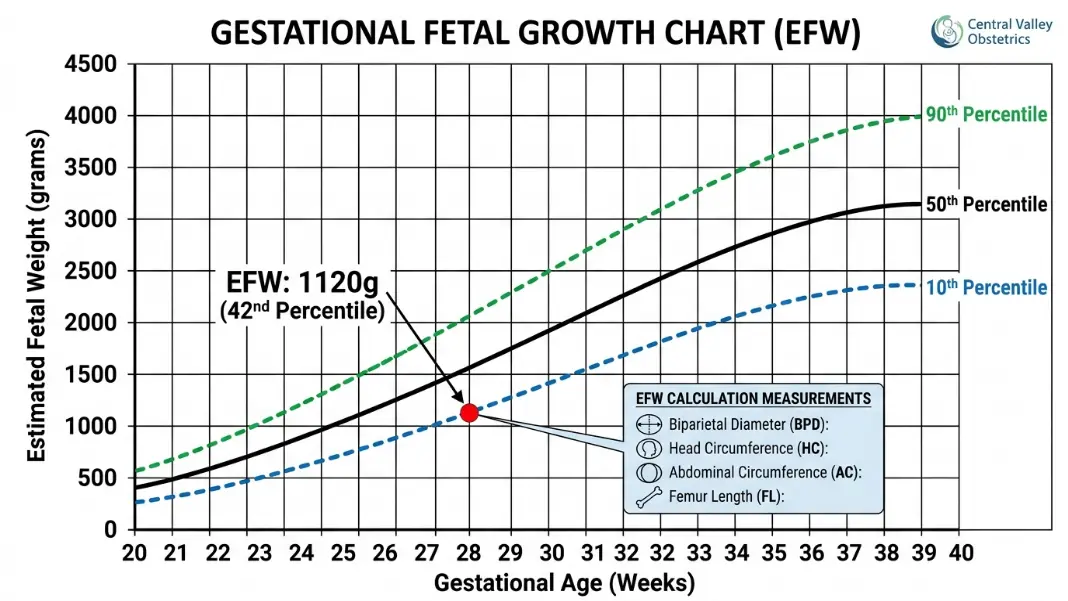
Fetal weight cannot be measured directly. Ultrasound estimates it by measuring four structures: head circumference (HC), biparietal diameter (BPD), abdominal circumference (AC), and femur length (FL). These four values are entered into a validated formula, with the Hadlock formula (1985) being the most widely used in American obstetric practice.
Estimated Fetal Weight (Hadlock) uses HC, BPD, AC, and FL in a log-scale equation
→ Result is compared to a fetal reference population at the same gestational week
→ Output is an estimated fetal weight percentile
The resulting estimated fetal weight (EFW) is then compared to a reference population to produce a percentile. Two reference populations are in common use. The Hadlock reference (United States, 1991) is the default in many American practices. The INTERGROWTH-21st standard (multinational, 2014) is the fetal equivalent of the WHO postnatal standard: built from optimally healthy pregnancies across 8 countries. The same estimated fetal weight can produce different percentile readings on these two charts. Your OB or sonographer can tell you which one is in use.
Sources of estimation error that matter in practice:
The EFW formula carries a known margin of error of plus or minus 15 to 20% in a normally progressing pregnancy. A fetus estimated at 2,000 grams could realistically weigh anywhere from 1,700 to 2,300 grams. That is a range of 600 grams, which can span several percentile levels at any given gestational age.
Abdominal circumference is the single measurement that most drives the EFW calculation and also the most difficult to capture precisely, particularly in the third trimester when the fetus is larger and less mobile. Two sonographers measuring the same fetus on the same day can produce abdominal circumference readings that differ by 5 to 10 mm, which translates to a meaningful shift in the percentile output. This measurement variability is why serial growth scans require at least 2 to 3 weeks between assessments to detect a real growth change versus noise.
Baby Percentile Week by Week: What Each Trimester Scan Shows
Fetal growth is not linear across pregnancy. The rate of weight gain accelerates significantly in the third trimester, which means the same absolute difference in weight carries a different percentile implication at 24 weeks versus 36 weeks.
Most practices structure growth surveillance around specific gestational windows.
| Gestational Week | Scan Purpose |
|---|---|
| 18 to 22 weeks | Anatomy scan: first detailed size measurements, organ structure review |
| 28 to 32 weeks | Third-trimester growth check: most predictive for growth restriction detection |
| 34 to 36 weeks | Additional assessment in higher-risk pregnancies |
| 38 to 40 weeks | Biophysical profile and amniotic fluid assessment when indicated |
The anatomy scan at 18 to 22 weeks produces a percentile reading, but it is the least predictive of any growth outcome. Fetal growth restriction, the main concern with low percentile, typically becomes apparent after 28 weeks when the fetus is in the most rapid phase of weight accumulation. The third-trimester scan at 28 to 32 weeks carries the most clinical weight.
A fetus consistently measuring at the 28th percentile at all three scans is tracking normally for a smaller baby. A fetus who was at the 50th at 20 weeks and drops to the 18th by 32 weeks shows a falling trajectory, which triggers a different clinical response than a stable low reading.
What normal variation looks like across scans:
Fetal percentile can shift 10 to 15 points between appointments without representing any genuine growth problem. Most of that shift is measurement variability, not a real change in the baby's growth rate. This is why growth restriction is not diagnosed from a single low reading but from a confirmed trend across serial scans, combined with Doppler blood flow assessment.
The question your OB is tracking is not "what is the percentile today?" but "is the estimated fetal weight increasing at a rate consistent with this gestational age?"
For context on how postnatal percentile charts work and what a stable versus declining trajectory looks like after birth, the Baby Weight Percentile Chart by Age includes the full WHO reference values month by month, which gives a useful baseline for understanding the difference between fetal and postnatal growth tracking.
How to Increase Baby Percentile During Pregnancy: What Has Evidence
This question is one of the most searched topics in prenatal nutrition forums. The honest answer is that the interventions available to a pregnant person in a low-risk, normal-growth pregnancy are fewer than many guides suggest, and the ones with actual evidence are fairly basic.
What has documented effect on fetal growth:
Adequate caloric intake during the second and third trimesters supports fetal weight gain. The American College of Obstetricians and Gynecologists (ACOG) recommends an additional 340 calories per day in the second trimester and 450 per day in the third, on top of pre-pregnancy maintenance calories. Protein is the dietary component most directly associated with fetal tissue development. Third-trimester protein intake of 70 to 100 grams per day is the recommended range.
Stopping smoking, if applicable, is the single intervention with the most consistent evidence for improving fetal growth outcomes. Smoking directly reduces uteroplacental blood flow through vasoconstriction. Cessation at any gestational age is associated with improved fetal weight outcomes, with earlier cessation producing the greatest benefit.
Iron deficiency anemia, identified through low ferritin on prenatal labs, is associated with reduced birth weight through impaired oxygen transport to the placenta. Correction with supplementation when indicated has documented effects on fetal growth outcomes.
What does not affect fetal percentile in a normal pregnancy:
Consuming large quantities of specific foods, taking supplements beyond recommended levels, and increasing physical activity have no documented effect on fetal percentile when fetal growth is already progressing normally. If fetal growth restriction is caused by placental insufficiency, dietary adjustments cannot compensate for reduced uteroplacental blood flow. In those cases, increased monitoring and delivery timing decisions are the clinical tools, not nutrition changes.
The What Does Baby Percentile Mean guide covers how postnatal percentile is calculated after birth and what the WHO standard considers normal for the first 24 months, which is useful context for how fetal and postnatal measurements relate.
When a Low Fetal Percentile Becomes a Clinical Concern: SGA and FGR
Two terms come up when fetal percentile is low, and they are not interchangeable.
Small for gestational age (SGA) is a statistical description. It means the estimated fetal weight is below the 10th percentile for gestational age and sex. SGA is not a diagnosis. A fetus at the 8th percentile born to petite parents who both have small frames is constitutionally small, not growth restricted. The percentile falls below the threshold, but the baby is growing exactly as genetics predict.
Fetal growth restriction (FGR), also called intrauterine growth restriction (IUGR), is a clinical diagnosis. It means the fetus is not reaching its genetic growth potential due to a pathological cause, most commonly uteroplacental insufficiency. FGR is identified through a falling growth trajectory, abnormal Doppler blood flow in the umbilical artery, and sometimes reduced amniotic fluid volume. A fetus can be SGA without FGR, and can show FGR signs while still above the 10th percentile if their personal trajectory is declining significantly.
Monitoring thresholds used in obstetric practice:
These are general guidelines; individual practices and high-risk maternal-fetal medicine specialists may use different protocols.
| EFW Percentile Zone | Typical Clinical Response |
|---|---|
| 10th to 20th | Increased surveillance; growth scan in 3 to 4 weeks |
| 5th to 10th | More frequent monitoring; umbilical artery Doppler assessment |
| Below 5th | Intensive monitoring; early delivery planning discussion |
| Falling trajectory (any percentile) | Immediate reassessment regardless of absolute level |
Doppler assessment of umbilical artery blood flow is the key investigation that separates a constitutionally small fetus from one with impaired placental function. Normal Doppler flow in a fetus below the 10th percentile significantly reduces clinical concern.
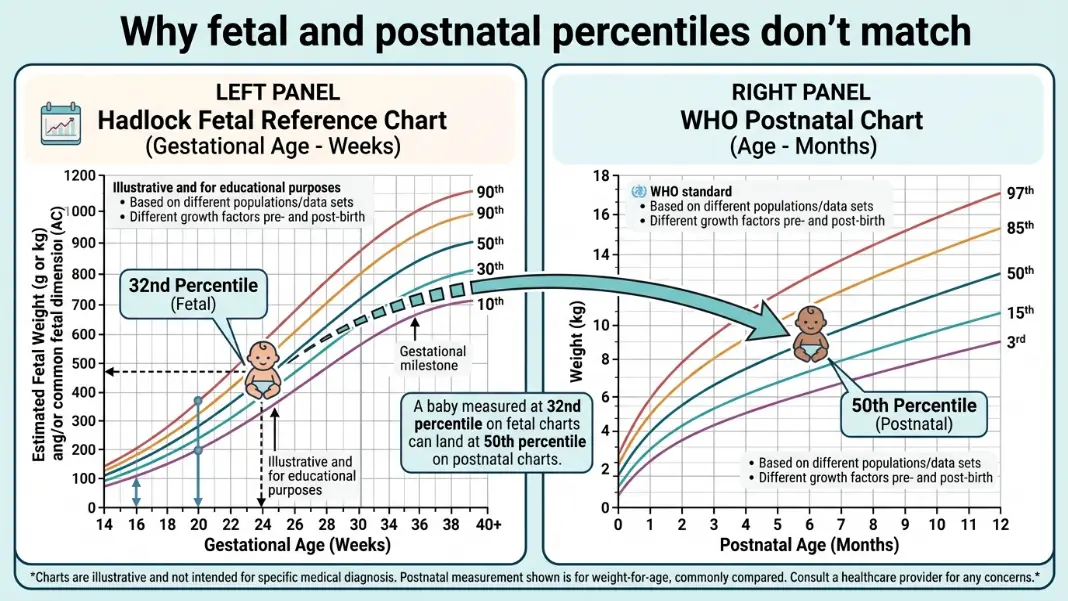
Fetal Percentile vs. Postnatal Percentile: Why the Numbers Rarely Match
Many parents notice their baby arrives in a different percentile than the ultrasound predicted. This is normal and expected for two distinct reasons, and understanding them removes the confusion.
First, the reference populations differ. Fetal percentiles use either the Hadlock or INTERGROWTH-21st reference. Postnatal percentiles use the WHO Child Growth Standards, built from a different sample using different methodology at a different time period. A fetus at the 32nd percentile on the Hadlock reference is not at the 32nd on the WHO postnatal chart by definition. The two charts share a name for the concept but do not share a scale.
Second, measurement accuracy is fundamentally different. Fetal weight is estimated from 4 ultrasound measurements with a plus or minus 15 to 20% error margin. Postnatal weight is measured directly on a calibrated scale. The direct measurement is far more reliable than the estimate. A baby's actual birth weight often falls outside the predicted range from the third-trimester scan, which is expected given the error margin in the formula.
The practical implication: if fetal percentile was low throughout pregnancy but your baby was born at a weight that places them in the 40th percentile on the WHO chart and they are tracking normally across early well-child visits, the postnatal chart is now the correct reference. Use the Baby Percentile Calculator for postnatal tracking from birth through 24 months using the WHO standard.
Baby percentile during pregnancy is estimated fetal weight compared to other fetuses at the same gestational age. It is calculated from four ultrasound measurements (head circumference, biparietal diameter, abdominal circumference, femur length) using a formula like Hadlock, then matched against a fetal reference population. The result carries an error margin of plus or minus 15 to 20%, which is why fetal percentile often does not match the postnatal WHO percentile after birth. The two systems use different methods and different reference populations.
The evidence-based interventions for supporting fetal growth are adequate caloric intake (an extra 340 to 450 calories per day in the second and third trimesters), sufficient protein intake (70 to 100 grams per day in the third trimester), stopping smoking if applicable, and treating iron deficiency anemia if identified in prenatal labs. Eating specific foods, taking extra supplements beyond recommended levels, or increasing exercise have no documented effect on fetal percentile in a normally progressing pregnancy. When FGR is caused by placental insufficiency, diet cannot compensate for reduced blood flow.
Any fetal percentile from the 10th to the 90th is considered normal by most obstetric guidelines. Below the 10th qualifies as small for gestational age (SGA) and typically triggers increased growth monitoring, though SGA alone is not a diagnosis of a problem. What matters as much as the absolute number is whether the trajectory is stable. A fetus consistently at the 12th percentile across three scans is less concerning than one who was at the 50th at 20 weeks and fell to the 18th by 32 weeks.
Fetal percentile is calculated during ultrasound by measuring head circumference, biparietal diameter, abdominal circumference, and femur length. The sonographer enters these into an estimation formula (usually Hadlock) to produce an estimated fetal weight. That weight is compared to a reference population at the same gestational week, and the percentile result appears on the scan report alongside the estimated weight. Your sonographer or OB can read it directly from the report.
Small for gestational age (SGA) means estimated fetal weight is below the 10th percentile for gestational age. It is a statistical description, not a clinical diagnosis. Fetal growth restriction (FGR) means the fetus is failing to reach its genetic growth potential due to an underlying cause, most often placental insufficiency. A fetus can be SGA without FGR if they are constitutionally small. FGR is identified through a falling growth trajectory, abnormal umbilical artery Doppler flow, or reduced amniotic fluid volume, not a single low percentile reading.
A dropping fetal percentile between 20 and 36 weeks can reflect real growth slowing, normal measurement variability, or both. Ultrasound EFW estimates have a 15 to 20% error margin, so a drop of 10 to 15 percentile points between scans can fall within normal measurement noise rather than indicating a real change. A genuine downward trend is more reliably identified when serial scans across at least 3 measurements taken 2 to 3 weeks apart all show consistent decline. Your OB will pair the percentile trend with Doppler blood flow assessment to distinguish measurement variability from true growth restriction.
Written by
Hassaan Rasheed
Web Developer & Content Researcher
Hassaan builds calculators and writes research-backed guides on finance, math, payroll, and construction topics. Every number in his articles is sourced from official data and worked through by hand.
View LinkedIn Profile