99th Percentile Baby: What High and Low Percentiles Mean (2026)
99th percentile baby weighs more than 99% of same-age infants. What high and low percentile actually means clinically, when it matters, and when it doesn't.
When the nurse says your baby is in the 99th percentile, most parents hear one of two things: "great job" or quiet worry about whether their baby is too large. The actual clinical interpretation is neither of those. A 99th percentile reading means your baby is larger than 99 out of 100 same-age babies in the WHO reference population. It does not mean your baby is overweight, and it does not mean there is a problem.
What it means in practice depends on whether that reading has been consistent across multiple visits or whether it appeared suddenly. Use the Baby Percentile Calculator to track weight and length over time. A single extreme reading tells a clinician almost nothing. A pattern of readings at the same extreme tells them something specific.
What the 99th and 98th Percentile Mean for a Baby's Weight
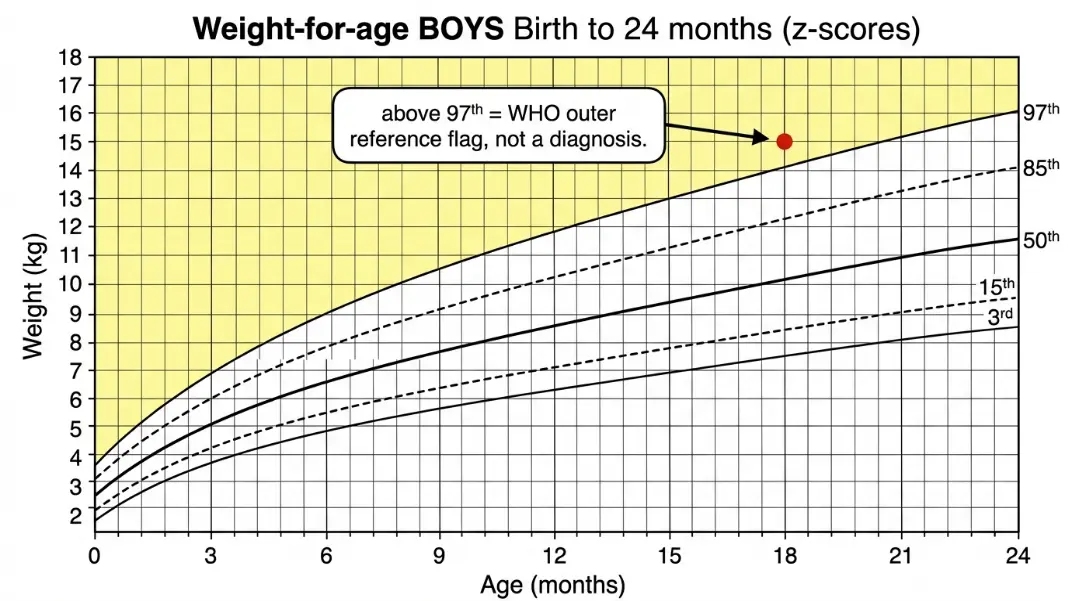
A baby at the 99th percentile for weight weighs more than 99% of babies the same age and sex in the WHO reference population. At 6 months, the 97th percentile weight for boys is approximately 9.3 kg (20.5 lb). The 99th percentile sits above that. These babies are large by any comparison.
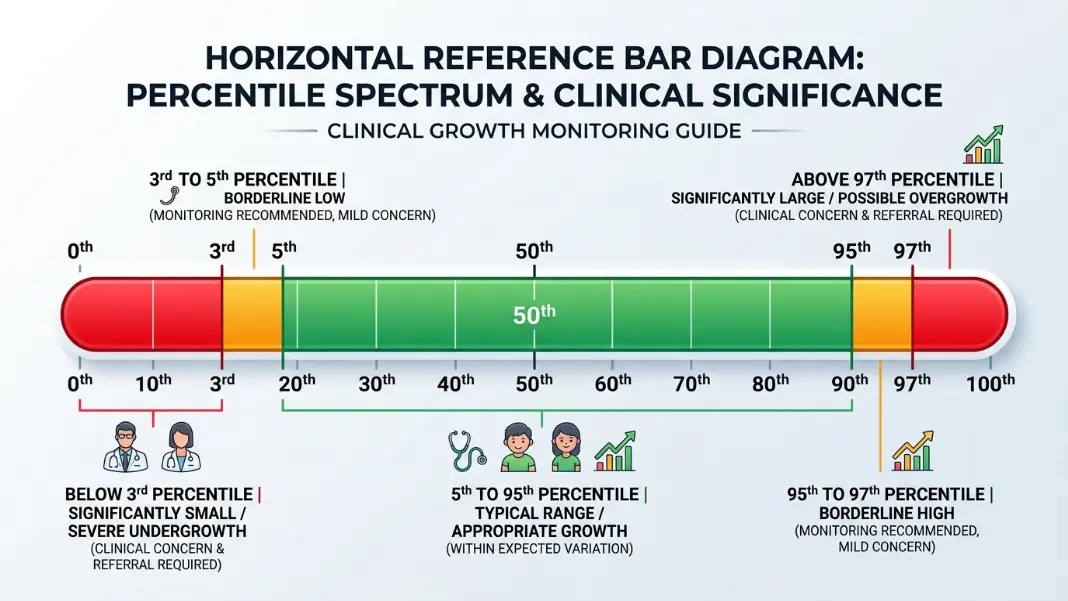
Above the 97th percentile is the WHO's outer flagging threshold. Readings above the 97th appear on WHO growth monitoring protocols as outside the reference range, which is a statistical designation, not a medical diagnosis. A single reading above the 97th does not diagnose a problem.
When a high percentile is not a concern:
Large babies of large parents are the most common explanation for consistently high percentile readings. If both parents are tall with large frames, a baby tracking at the 95th or 97th throughout infancy is probably expressing genetic size, not overfeeding. Family history is the first thing a pediatrician considers when a baby measures consistently above the 90th.
Exclusively breastfed babies have a natural limit on intake because breastfeeding self-regulates more effectively than bottle feeding. A breastfed baby in the 98th percentile who gained weight rapidly in the first 3 months and then began to plateau is showing the normal trajectory for a large breastfed infant. This pattern does not indicate a problem.
Some parents of babies with consistently high postnatal percentiles notice that fetal percentile during pregnancy was also high. The two measurements use different reference populations and methods, but a pattern of large size that started in the third trimester and continues after birth is typically genetic rather than pathological. The Baby Percentile During Pregnancy guide covers how fetal percentile is estimated and why it often differs from the postnatal reading.
When a high percentile warrants a closer look:
A rapid upward crossing of percentile lines is more clinically significant than a consistently high reading. A baby who was at the 50th at birth and has risen to the 97th by 4 months, gaining weight at a rate noticeably faster than the reference curves, is showing an accelerating trajectory. The change is what matters, not just the number.
The Baby Weight Percentile Chart by Age has the full WHO reference values at all 9 percentile levels for each month, which lets you compare your baby's trajectory against the published curves rather than a single reading.
What the 3rd Percentile Means and When It Becomes a Concern
A baby at the 3rd percentile for weight weighs more than only 3% of babies the same age and sex. Below the 3rd percentile is outside the WHO reference range on the lower end, the same way above the 97th is on the upper end.
The critical distinction is whether a baby at the 3rd percentile has always been at the 3rd or arrived there recently.
Constitutionally small babies:
A baby whose birth weight placed them at the 5th percentile and who tracks consistently between the 3rd and 8th throughout infancy is almost certainly constitutionally small. They are small because their genetics predict small. Both parents are likely smaller than average. The baby is not failing to grow; they are growing exactly on their curve. Pediatricians confirm this by checking the growth trend and asking about parental height and build.
Babies who fall to the 3rd:
A baby who was at the 35th percentile at birth and drops to the 3rd by 6 months has crossed several major percentile lines. That trajectory is the concerning pattern, regardless of the final percentile number. The drop indicates the baby is not gaining weight at the expected rate. Causes range from inadequate intake (feeding difficulty, low milk supply, latch problems in breastfed infants) to underlying medical conditions affecting absorption or metabolism.
The clinical term for this pattern is failure to thrive (FTT), now more commonly called pediatric undernutrition or growth faltering in current guidelines. The emphasis is on the trend, not on being below a fixed threshold.
The Difference Between High and Low Percentile in Clinical Practice
High and low extreme percentile readings are evaluated on the same framework: the trajectory matters more than the absolute position.
This table shows the key difference in how clinicians interpret the two extremes.
| Reading | Most Common Explanation | When It Raises Concern |
|---|---|---|
| Consistently above 95th | Genetic large size | Rapid upward crossing of lines; early puberty signs |
| Single reading above 97th | Genetic size; measurement timing | Usually not; reassess at next visit |
| Consistently below 5th | Genetic small size | Usually not if stable and parents are small |
| Single reading below 3rd | Illness; recent reduced intake | Check trend at next visit; assess feeding |
| Crossing 2+ lines downward | Feeding difficulty; growth faltering | Immediate clinical assessment |
| Crossing 2+ lines upward | Growth acceleration | Less common; assess in context |
The phrase "crossing two major percentile lines" is the standard benchmark in pediatric growth literature for when a trend change becomes clinically significant. Major lines are the 3rd, 10th, 25th, 50th, 75th, 90th, and 97th.
What the 95th percentile means compared to the 99th:
The 95th percentile is the standard upper boundary of the clinically normal range. A baby at the 94th percentile is described as within normal range. A baby at the 96th is above the upper boundary. In practice, a baby stable at the 96th with normal length-to-weight proportions is treated very similarly to one at the 90th. The thresholds are reference points, not hard clinical cutoffs.
A baby at the 99th or above the 99th is statistically unusual enough that the visit usually includes a question about whether the trajectory has been consistent. Stable 99th-percentile tracking from birth, in a large-framed family, typically ends the conversation. A jump to the 99th from the 60th in two months does not.
How High Percentile and Low Percentile Relate to Length-for-Age
Weight percentile in isolation tells only part of the story. Length percentile is the other variable, and the relationship between the two matters clinically.
A baby at the 95th percentile for weight and the 95th for length is large proportionately. Their weight is appropriate for their size. A baby at the 95th percentile for weight and the 50th for length has weight that is significantly high relative to their length. These two pictures are clinically different, even though the weight percentile is identical.
The same logic applies at low percentiles. A baby at the 5th for weight and the 5th for length is proportionately small. A baby at the 5th for weight and the 60th for length is carrying significantly less weight than expected for their height, which is more concerning.
Pediatricians evaluate the weight-to-length relationship at every well-child visit alongside the individual percentile readings. For babies and toddlers under 24 months, weight-for-length is the equivalent of BMI in older children and adults. It contextualizes the weight reading within the baby's frame.
The What Does Baby Percentile Mean guide explains how weight and length percentiles are calculated separately and why the two measurements are always tracked together.
What to Expect at Visits When Percentile Is at an Extreme
A pediatrician's response to a baby at the 99th or the 3rd percentile follows a predictable framework. Understanding that framework makes the conversation more productive.
At a very high percentile visit, your pediatrician is likely to:
- Review the growth chart from prior visits to confirm the trajectory
- Ask about family history: parent heights, build, birth weights of siblings
- Ask about feeding method, frequency, and whether feedings are self-regulated
- If breastfed, assess whether feeds are to satiety or on a rigid schedule
- If formula fed, check concentration and daily volume
- Assess length percentile to see whether weight and length are proportionate
A baby tracking consistently above the 95th with proportionate length and a large-framed family is typically followed on standard well-child schedule without additional intervention.
At a very low percentile visit, your pediatrician is likely to:
- Review whether the current reading is consistent with prior visits or a new drop
- Ask about feeding: how often, how much, signs of hunger or satiety
- Ask about wet and dirty diaper frequency as an output measure of intake
- Check length percentile to assess weight-for-length ratio
- If this is a new drop, schedule a follow-up weight check within 2 to 4 weeks rather than waiting for the next well-child appointment
If a downward trend across multiple visits is confirmed, the next steps depend on the clinical picture: feeding assessment with a lactation consultant or feeding therapist, dietary changes, or referral for further evaluation of absorption and metabolism.
A baby at the 99th percentile for weight weighs more than 99% of babies the same age and sex in the WHO reference population. It means the baby is very large by statistical comparison. Above the 97th percentile is outside the WHO reference range, which is a statistical flag, not a diagnosis. A consistently large baby from large parents, with proportionate length, is typically just genetically large. The concerning pattern is a rapid rise from a normal percentile to above the 97th across just a few visits.
Not necessarily. Being in the 99th percentile for weight does not mean a baby is overweight. Pediatricians assess weight in relation to length using the weight-for-length ratio. A baby at the 99th for weight who is also at the 97th for length has proportionate measurements for a large-framed baby. A baby at the 99th for weight and the 50th for length carries significantly more weight than expected for their length, which may warrant a closer look at feeding patterns. Family size and growth trajectory matter more than a single percentile number.
A baby at the 3rd percentile for weight weighs more than only 3% of same-age babies in the WHO reference population. Below the 3rd percentile is outside the WHO reference range. A baby who has always tracked near the 3rd percentile and has small parents is most likely constitutionally small. A baby who drops from the 40th to the 3rd across several visits has crossed multiple major percentile lines, which is clinically significant regardless of the final number and warrants a feeding and growth assessment.
The 98th percentile for baby weight means your baby weighs more than 98 out of 100 babies the same age and sex in the WHO reference population. The WHO publishes reference tables at the 97th percentile as the highest standard threshold, so the 98th falls just above the published outer boundary. Clinically, it is treated the same as a reading above the 97th: stable tracking with proportionate length in a large-framed family is typically not a concern, while a rapid rise from a mid-range percentile warrants review.
The most important warning pattern is a downward shift of two or more major percentile lines across multiple visits, for example dropping from the 75th to the 25th over two or three appointments. A single low or high reading after an illness or growth spurt is usually not significant. Any reading below the 3rd or above the 97th that appears suddenly, rather than tracking there consistently from birth, warrants a conversation with your pediatrician. Stable tracking at any percentile, high or low, is almost always more reassuring than a trend in either direction.
The 95th percentile is the standard upper boundary of the clinical normal range used by the American Academy of Pediatrics. A baby above the 95th is above the normal threshold but below the WHO outer reference limit at the 97th. The 99th percentile is above the 97th WHO reference boundary, placing the baby in the extreme upper range statistically. In practice, the clinical evaluation is similar for both: check length-to-weight proportionality, review the growth trajectory, and consider family size before drawing any conclusions.
Written by
Hassaan Rasheed
Web Developer & Content Researcher
Hassaan builds calculators and writes research-backed guides on finance, math, payroll, and construction topics. Every number in his articles is sourced from official data and worked through by hand.
View LinkedIn Profile