Corrected Calcium Formula: How to Adjust for Low Albumin (2026)
Total serum calcium is unreliable when albumin is low. The Payne correction formula adjusts for protein binding. When to use it and when ionized calcium is better.
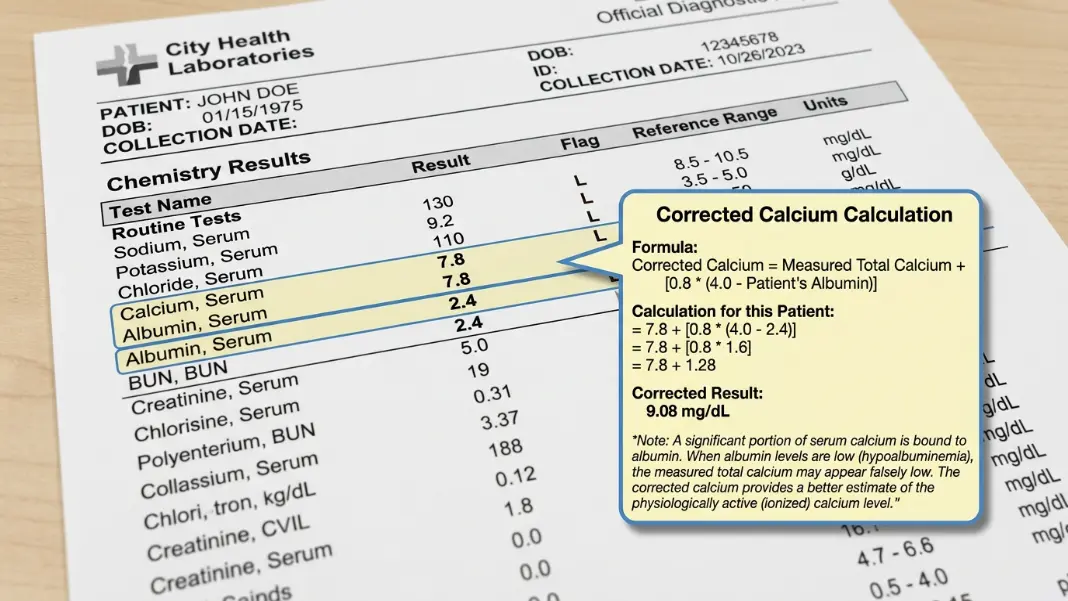
A patient's total serum calcium comes back at 7.8 mg/dL. That looks like hypocalcemia. But if albumin is 2.4 g/dL instead of the normal 4.0, the calcium is artificially low because less albumin means less protein-bound calcium. The actual free (ionized) calcium may be perfectly normal. Without correcting for albumin, you are reading a lab artifact, not a clinical finding.
Use the Corrected Calcium Calculator to run the adjustment in seconds. This guide explains the formula, why protein binding matters, when the correction is appropriate, and when you need direct ionized calcium measurement instead.
The Corrected Calcium Formula
The most widely used correction is the Payne formula, published in 1973:
Corrected Calcium (mg/dL) = Measured Calcium (mg/dL) + 0.8 x (4.0 - Albumin g/dL)
Worked example:
- Measured calcium: 7.8 mg/dL
- Albumin: 2.4 g/dL
Corrected calcium = 7.8 + 0.8 x (4.0 - 2.4) = 7.8 + 0.8 x 1.6 = 7.8 + 1.28 = 9.08 mg/dL
That is within the normal range of 8.5 to 10.2 mg/dL. The apparent hypocalcemia disappears once albumin is accounted for. Acting on the uncorrected value would lead to unnecessary workup or treatment.
The math works in both directions. If albumin is elevated above 4.0 g/dL (uncommon), the correction subtracts from measured calcium. Each 1 g/dL change in albumin shifts measured total calcium approximately 0.8 mg/dL in the same direction.
The 4.0 g/dL reference point is the mean albumin used when calcium normal ranges were established. All reference ranges were derived from patients with normal albumin, so the correction effectively brings a hypoalbuminemic patient into that same reference population.
Why Albumin Affects Serum Calcium
Calcium in the blood exists in three forms. About 50% is ionized (free), which is the biologically active fraction that affects nerve conduction, muscle contraction, and cardiac function. Roughly 40% is protein-bound, mostly to albumin. The remaining 10% is complexed with anions such as phosphate, citrate, and bicarbonate.
Total serum calcium measures all three fractions combined. When albumin drops, the protein-bound fraction drops proportionally. But ionized calcium is tightly regulated by parathyroid hormone (PTH) and stays within range even as total calcium falls.
This is common in hospitalized patients. Conditions that lower albumin and therefore lower total calcium without affecting ionized calcium include:
- Liver disease (reduced albumin synthesis)
- Nephrotic syndrome (albumin lost in urine)
- Protein-calorie malnutrition
- Critical illness or sepsis (capillary leak and fluid shifts dilute albumin)
- Large-volume IV fluid resuscitation
In all these settings, an uncorrected total calcium systematically underestimates the patient's true calcium status. The Payne correction restores the value to what it would be at normal albumin.
Corrected Calcium vs Ionized Calcium
The Payne formula is an estimate. Direct measurement of ionized calcium is more accurate and needs no correction.
| Method | Accuracy | Best Use Case |
|---|---|---|
| Total calcium (uncorrected) | Poor when albumin is abnormal | Screening in otherwise healthy outpatients |
| Corrected calcium (Payne) | Reasonable in most outpatient settings | Hypoalbuminemic patients, routine labs |
| Ionized calcium (direct) | Best in all cases | ICU, acid-base disorders, critical illness |
When to order ionized calcium instead of relying on the correction:
- ICU patients, particularly those with sepsis, vasopressors, or rapid volume resuscitation
- Patients with significant acid-base disturbances (pH changes alter albumin binding affinity, which the formula does not account for)
- Multiple myeloma or other paraproteinemias (abnormal immunoglobulins also bind calcium; the formula only adjusts for albumin)
- When clinical symptoms and corrected calcium disagree
- Pre- and post-parathyroid surgery
Ionized calcium requires a separate tube or direct arterial/venous sample and is measured by blood gas analyzer. It is slightly more expensive and not always available in outpatient settings, which is why the Payne correction remains the practical default for routine labs.
Normal Ranges and What Abnormal Values Mean
Normal corrected calcium: 8.5 to 10.2 mg/dL (2.12 to 2.55 mmol/L in SI units).
To convert mg/dL to mmol/L: divide by 4.008.
Hypocalcemia (corrected calcium below 8.5 mg/dL):
| Severity | Corrected Calcium | Clinical Findings |
|---|---|---|
| Mild | 7.5 to 8.5 mg/dL | Often asymptomatic; perioral tingling |
| Moderate | 6.5 to 7.5 mg/dL | Muscle cramps, Chvostek sign, Trousseau sign |
| Severe | Below 6.5 mg/dL | Tetany, laryngospasm, prolonged QTc, seizures |
Common causes: hypoparathyroidism, vitamin D deficiency, hypomagnesemia (blocks PTH secretion), pancreatitis, hungry bone syndrome after parathyroidectomy.
Hypercalcemia (corrected calcium above 10.2 mg/dL):
Clinically summarized as "bones, stones, groans, moans": bone pain, kidney stones, gastrointestinal symptoms (nausea, constipation), and neuropsychiatric changes (fatigue, confusion, depression). Primary hyperparathyroidism and malignancy together account for over 90% of hypercalcemia cases.
When the Payne Formula Does Not Apply
The correction is a population-based estimate, not an exact ionized calcium value. Several situations limit its reliability.
Variable correction factor: The 0.8 coefficient is a statistical mean. Individual patients differ; some have a true correction factor of 0.7, others 1.0. The formula gives a reasonable approximation, not a precise ionized value.
Acid-base effects: Acidosis decreases albumin's binding affinity for calcium, so more calcium is free (ionized) than the total would suggest. Alkalosis increases binding affinity, leaving less calcium free. The Payne formula ignores pH entirely. In a patient with metabolic alkalosis and a normal corrected calcium, the actual ionized calcium may be low. In acidosis, it may be normal or high despite a low corrected calcium. For any patient with a significant pH disturbance, measure ionized calcium directly.
Paraproteinemias: In multiple myeloma, Waldenström macroglobulinemia, and similar conditions, abnormal immunoglobulins also bind calcium. Total calcium overestimates ionized calcium in these patients because the correction only adjusts for albumin binding, not immunoglobulin binding. Direct ionized calcium is essential in these cases.
Critical illness: Multiple studies have demonstrated that the Payne formula performs poorly in ICU patients. Direct ionized calcium measurement has become standard of care in intensive care for this reason.
When clinical symptoms and corrected calcium do not match, trust the symptoms and order ionized calcium.
Corrected calcium (mg/dL) = measured calcium (mg/dL) + 0.8 x (4.0 - albumin in g/dL). This adjusts for the roughly 40% of serum calcium that is protein-bound to albumin. When albumin is below the normal reference of 4.0 g/dL, measured total calcium reads artificially low. The correction restores it to what it would be at normal albumin, making it comparable to standard reference ranges.
Use the Payne correction for routine outpatient labs in patients with known low albumin due to liver disease, malnutrition, or nephrotic syndrome. Order direct ionized calcium in ICU patients, patients with significant acid-base disorders, patients with multiple myeloma or paraproteinemias, and any time the corrected calcium does not match the clinical presentation. Ionized calcium is the gold standard; the Payne correction is a practical approximation when direct measurement is not available.
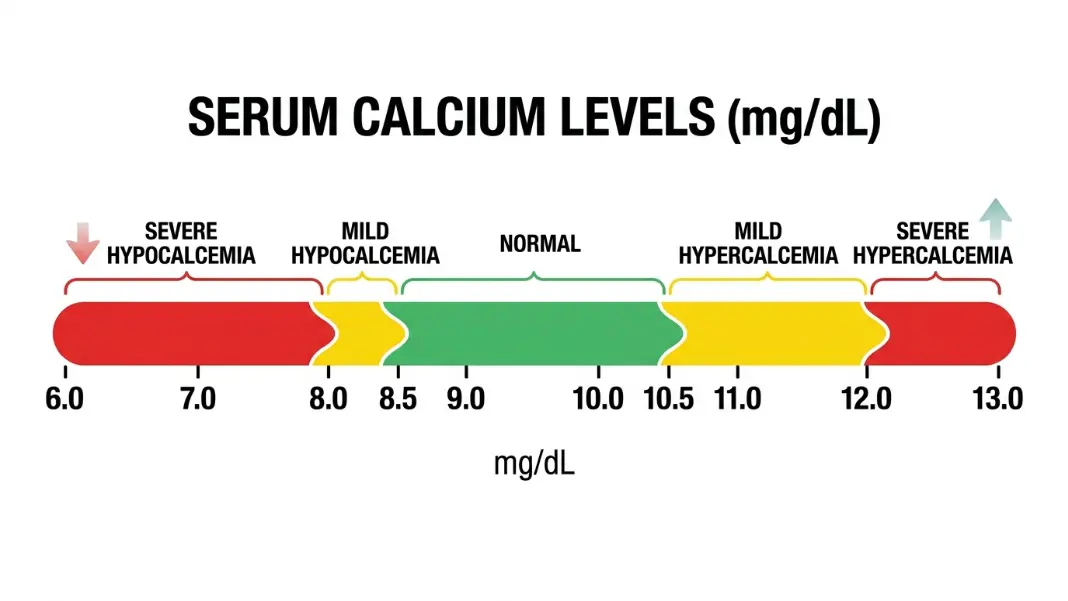
Normal corrected serum calcium is 8.5 to 10.2 mg/dL (2.12 to 2.55 mmol/L). Below 8.5 mg/dL is hypocalcemia; above 10.2 mg/dL is hypercalcemia. Severe hypocalcemia below 6.5 mg/dL carries risk of tetany, laryngospasm, and cardiac arrhythmia with prolonged QTc. Hypercalcemia above 12 mg/dL warrants urgent evaluation for malignancy or primary hyperparathyroidism.
About 40% of total serum calcium is protein-bound, mostly to albumin. When albumin falls, fewer binding sites exist, so measured total calcium drops even though free ionized calcium may be normal. PTH tightly regulates ionized calcium independently, so it stays in range while total calcium falls with albumin. Measuring only total calcium in a patient with low albumin gives a falsely low reading that does not reflect the biologically active calcium level.
The Payne formula does not account for pH. Alkalosis increases albumin's binding affinity for calcium, meaning more calcium is protein-bound and less is free. This can produce a normal corrected calcium alongside genuinely low ionized calcium. Acidosis decreases binding affinity, freeing more calcium, so ionized calcium can be normal or elevated even with a low total calcium. In patients with significant acid-base disturbances, direct ionized calcium measurement is more reliable than any correction formula.
No. Apply the Payne formula only to total serum calcium results. If your lab reports ionized calcium directly (measured by blood gas analyzer or ion-selective electrode), that value already reflects the free fraction and needs no albumin correction. Only apply the formula when the result is labeled "total calcium" or "serum calcium" and albumin is also abnormal.
Written by
Hassaan Rasheed
Web Developer & Content Researcher
Hassaan builds calculators and writes research-backed guides on finance, math, payroll, and construction topics. Every number in his articles is sourced from official data and worked through by hand.
View LinkedIn Profile